|
|||
Malignant
Disease: Staging
of Gynecologic Application
of Vaginal Application
of Uterine Afterloading Applicators Abdominal
Injection of Chromic Phosphate Radical
Vulvectomy Reconstruction
of the Transverse
Rectus Colonic
"J" Pouch Rectal Ileocolic Continent Urostomy (Miami Pouch) Construction
of Neoanus Skin-Stretching
System Versus Skin Grafting Gastric
Pelvic Flap for Control
of Hemorrhage in Gynecologic Surgery Repair
of the Punctured Ligation
of a Lacerated Hemorrhage
Control in Presacral
Space What
Not to Do in Case of Pelvic Hemorrhage |
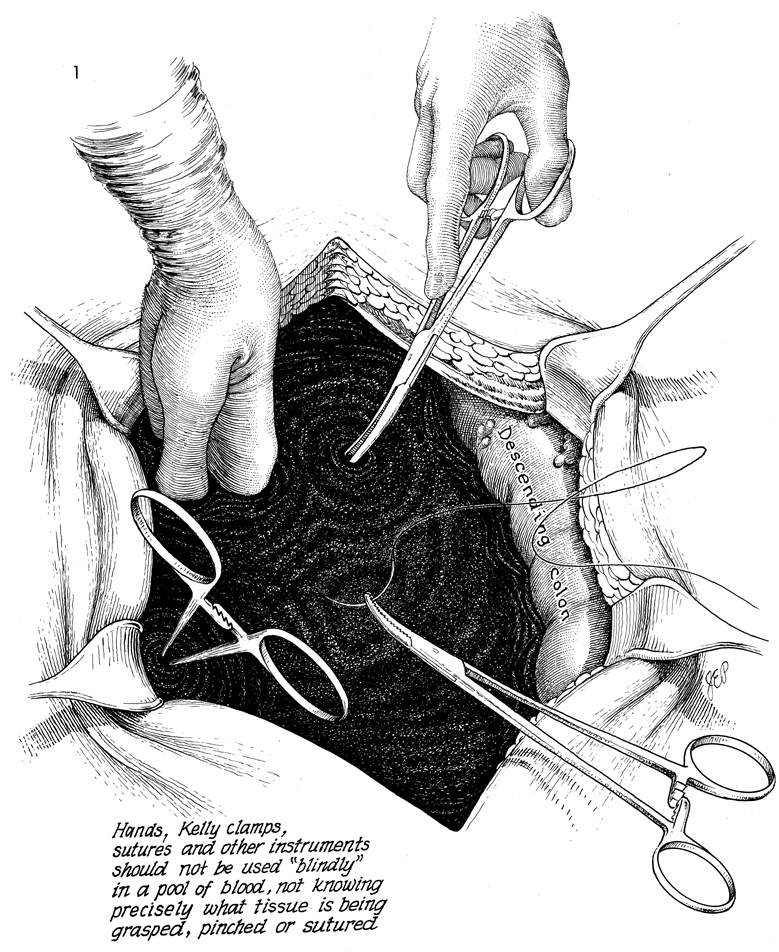
What Not to Do in Cases What not to do in cases of pelvic hemorrhage is important to the gynecologic surgeon. Laceration of a large pelvic vein, external iliac artery, external iliac vein, internal iliac artery, or internal iliac vein can produce copious hemorrhage that will fill the pelvis immediately (Fig. 1). Suction with location of the lacerations is the first step. Finger pressure is important and will stop the hemorrhage in most cases. What Not to Do. Nonvascular clamps such as the Kelly clamp crush arteries and veins and should not be used. Sutures on large needles placed blindly beneath the pool of blood not knowing precisely what tissue and what structure is being grasped, pinched, or sutured should not be used. Finger and pack pressure should be used until proper exposure of the vessel laceration can be made. This allows the operating room team to obtain proper vascular instruments, vascular suture, and cardiovascular needles. More damage can be created to the lacerated artery and vein by typical gynecologic clamps. Gynecologic suture and needles are frequently inappropriate in vascular surgery. Trying to place a suture in a hemorrhaging vein or artery is not a proper technique for repairing that artery or vein.
|
||

Copyright 2008 / Clifford R. Wheeless, Jr., M.D. and
Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.