
Uterus
Dilatation
and Curettage
Suction
Curettage
for Abortion
Management
of Major
Uterine Perforations
From Suction Curet or
Radium Tandem
Cesarean
Section
Myomectomy
Jones
Operation
for Correction of
Double Uterus
Hysteroscopic
Septal
Resection by Loop
Electrical Excision
Procedure (LEEP) for
Correction of a Double
Uterus
Manchester
Operation
Richardson Composite Operation
Total
Vaginal Hysterectomy
Total
Abdominal
Hysterectomy With
and Without Bilateral
Salpingo-oophorectomy
Laparoscopy-Assisted
Vaginal Hysterectomy |
Jones Operation for Correction
Of Double Uterus
The term "double uterus" in this atlas refers
to the various embryologic deformities resulting from failure of fusion
of the Mullerian ducts. Most patients with a double uterus have no
reproductive difficulties or fetal wastage and do not need surgical
intervention. Approximately 20%, however, have habitual first-or second-trimester
abortions.
Several procedures are available for correction of
the double-uterus deformity (Strassman, Tompkins, and Jones operations).
We have chosen to present the surgical details of the Jones operation
because in our opinion it is the most physiologic approach for the
correction of this deformity.
The purpose of the operation is to restore
the uterus to its normal configuration by removing the fibrous septum.
Physiologic Changes. The fibrous septum within a
double uterus makes a poor implantation site for the placenta. It lacks
the proper endometrial lining necessary to support nidation and placental
growth.
By removing this fibrous septum, the placenta grows on a normal, healthy
endometrium.
Points of Caution. Many obstetricians
prefer to deliver all of these patients by cesarean section at term
prior to labor.
Care must be taken to ensure that parallel incisions
into the fundus of the uterus are made to prevent cornual dissection
of the myometrium. Cornual dissection may jeopardize the intramural
portion of the Fallopian tube.
All of the fibrous septum must be removed.
Technique
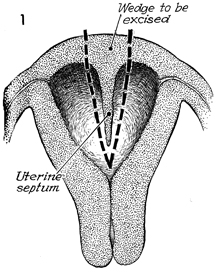
A frontal section of the uterus with the
uterine septum is shown. The dotted line indicates the
wedge to be excised. |
The patient is placed on the operating table
in the dorsal position. We have found it helpful to insert a
Foley catheter through the cervix into the endometrial cavity
and instill 10 mL of an indigo carmine solution to stain the
endometrial cavity prior to the uterine incision.
A second Foley catheter should
be inserted into the bladder.
The abdomen can be opened through
a midline or transverse incision. The bowel is packed away, and
a self-retaining retractor is used to keep the abdominal wound
open. The fundus is palpated with the thumb and index finger
to locate the extent of the fibrous septum. A traction suture
is placed in the midportion of the uterus. Additional traction
sutures are placed lateral to the fibrous septum.
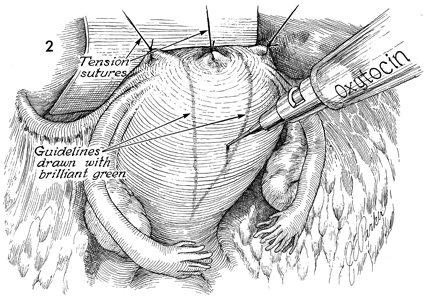
The myometrium
is injected at several points with a saline-Pitressin solution
(10 international units of Pitressin in 30 mL of saline solution).
Injection of this solution, which produces contraction of the
uterus, has been superior to applying a tourniquet to the lower
uterine segment for hemostasis. Regardless of the hemostatic
technique used (tourniquet or Pitressin injection), a bloodless
field in the operating wound is essential for meticulous dissection
and accurate placement of suture material. Brilliant green solution
is used to mark the lateral extent of the fibrous septum as determined
by palpation of the uterus. |
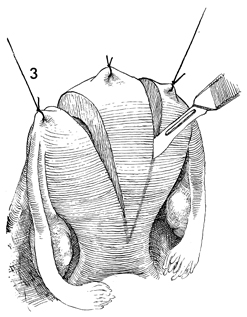
A scalpel is used to open the fundus along
the lines marked with brilliant green solution. Traction on the
three sutures is maintained by an assistant. Care must be taken
at this point so that lateral dissection of the myometrium into
the cornual area is avoided to prevent transection of the tube.
The entire fibrous septum must be excised. |
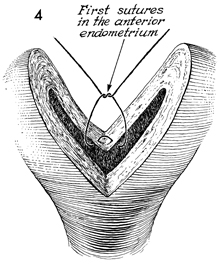
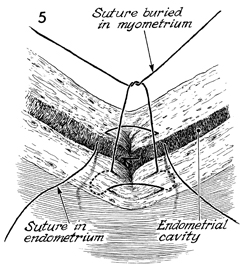
A row of 3-0 Dexon sutures
is placed through the endometrium, closing the endometrium and
the innermost layers of the myometrium. |
The second row of 2-0 Dexon is used to close
the myometrium with a mattress suture. |
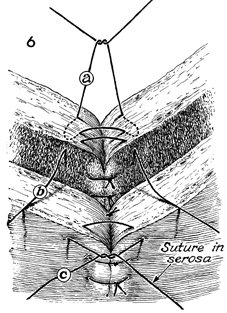
Figure 6 shows three layers
of sutures: those on the myometrium, (a), those on the
endometrium (b), and those on the serosa (c). |
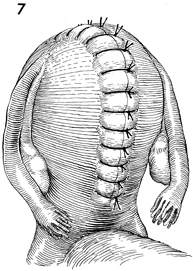
The completed operation is shown. Interrupted
sutures in the serosa have been placed approximately 1 cm apart
from the lower uterine segment of the opposite side. |
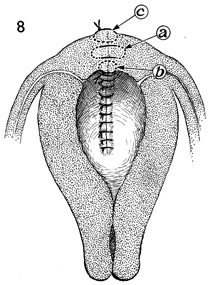
This frontal section of the uterus shows
the unified endometrial cavity. Sutures a, b and c have
been placed as described in Step 6. |
|
