|
||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
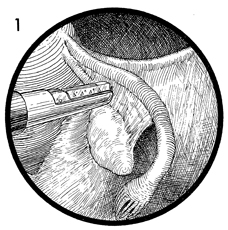
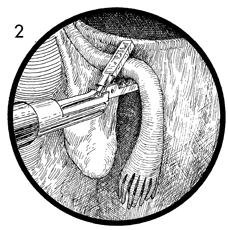
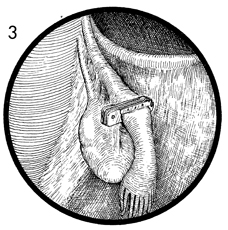
Hulka Clip Sterilization Laparoscopic Hulka clip application for female sterilization differs from the other methods of laparoscopy sterilization in that it applies a spring-loaded Silastic clip to the Fallopian tube. It has the advantage of producing the least tissue damage to the Fallopian tube and, therefore, may prove to be the most reversible form of female sterilization. The laparoscopic technique is the same as previously described for other laparoscopic procedures. The purpose of the operation is to effect female sterilization. Physiologic Changes. The oocyte and spermatozoa are prevented from meeting in the midportion of the Fallopian tube. Points of Caution. Care must be taken to ensure that the Hulka clip is over the entire Fallopian tube and that the tips of the clip grasp a small portion of mesosalpinx. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.