|
||||||||||
|
Diagnostic Uses of Laparoscopy Demonstration of Tubal Patency via Laparoscopy Laparoscopic Resection of Unruptured Ectopic Pregnancy Ovarian Biopsy via Laparoscopy Electrocoagulation of Endometriosis via Laparoscopy Lysis or Adhesions via Laparoscopy Control of Hemorrhage During Laparoscopy Sterilization by Electrocoagulation and Division via Laparoscopy Silastic Band Sterilization via Laparoscopy Hulka Clip Sterilization via Laparoscopy Sterilization by the Pomeroy Operation Sterilization by the Modified Irving Technique Sterilization by the Minilaparotomy Technique Sterilization - Ucheda Technique Tuboplasty - Microresection and Anastomosis of the Fallopian Tube |
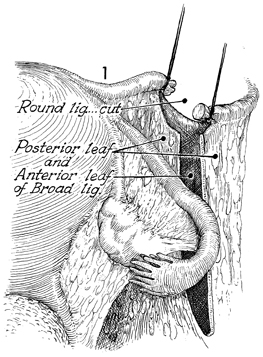
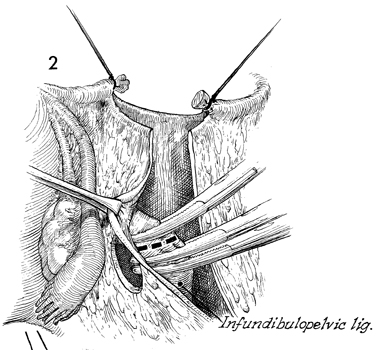
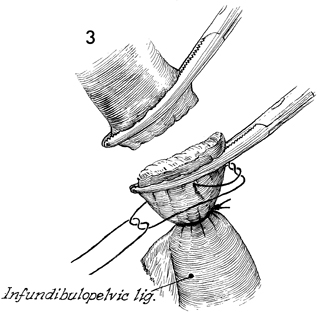
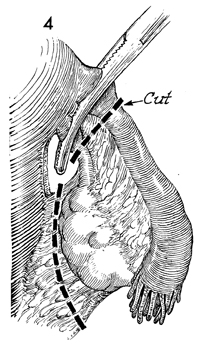
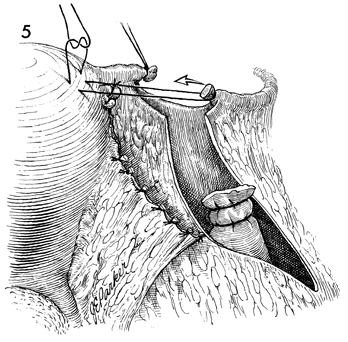
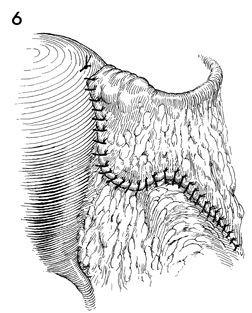
Salpingo-oophorectomy Salpingo-oophorectomy is needed when the disease process has invaded the Fallopian tube and ovary in such a manner that salvage of the ovary is undesirable or technically impossible. This occurs in both benign and malignant disease, particularly where the benefits derived from leaving the uterus and other adnexa in place outweigh the risks associated with the primary disease. The purpose of the operation is to remove the tube and ovary. Physiologic Changes. Although removal of one ovary may reduce the total hormone output, there is little clinical physiologic change. Points of Caution. The indundibulopelvic ligament must be dissected clear to the ureter if the ligament is to be clamped in the area of the pelvic brim. The infundibulopelvic ligament should be doubly tied because the venous network within this ligament tends to retract, producing hematomas that dissect up to the renal vessels. Transecting the round ligament and thus opening the broad ligament is not always necessary; however, it provides the most anatomic approach to this procedure and often allows a clean dissection of a tubo-ovarian mass without rupture. Technique
|
|||||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.