|
||||||||||||||||
|
Diagnostic Uses of Laparoscopy Demonstration of Tubal Patency via Laparoscopy Laparoscopic Resection of Unruptured Ectopic Pregnancy Ovarian Biopsy via Laparoscopy Electrocoagulation of Endometriosis via Laparoscopy Lysis or Adhesions via Laparoscopy Control of Hemorrhage During Laparoscopy Sterilization by Electrocoagulation and Division via Laparoscopy Silastic Band Sterilization via Laparoscopy Hulka Clip Sterilization via Laparoscopy Sterilization by the Pomeroy Operation Sterilization by the Modified Irving Technique Sterilization by the Minilaparotomy Technique Sterilization - Ucheda Technique Tuboplasty - Microresection and Anastomosis of the Fallopian Tube |
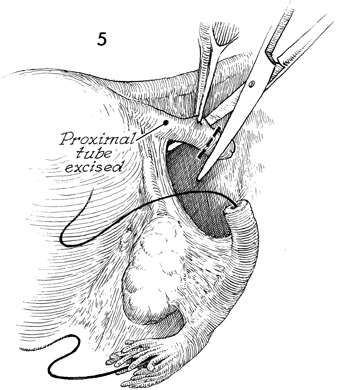
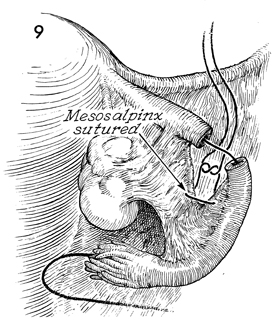
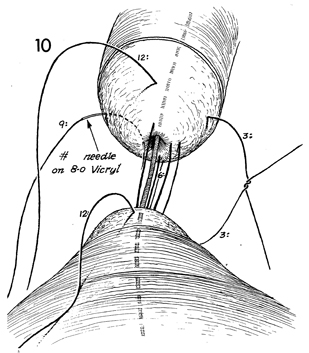
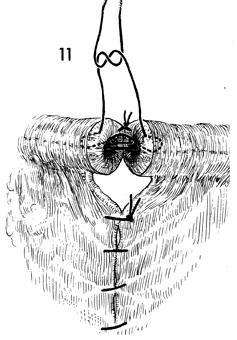
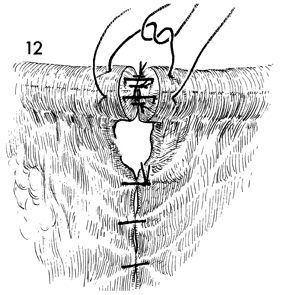
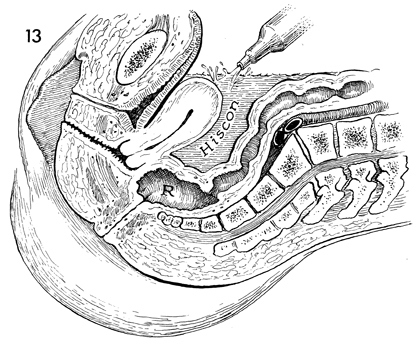
Tuboplasty
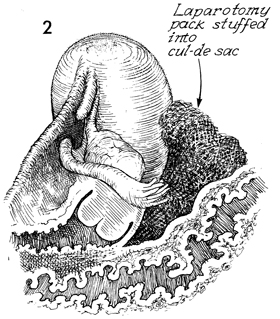
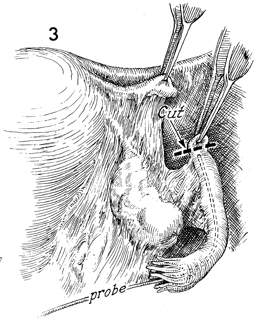
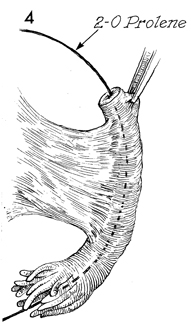
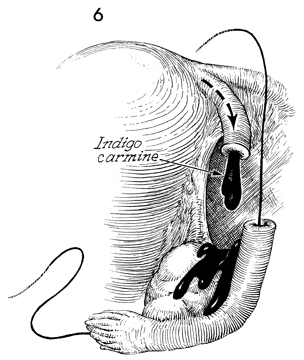
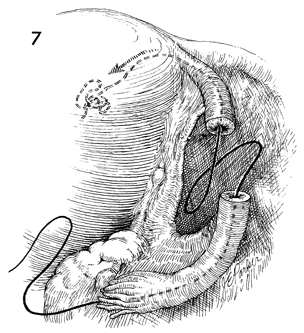
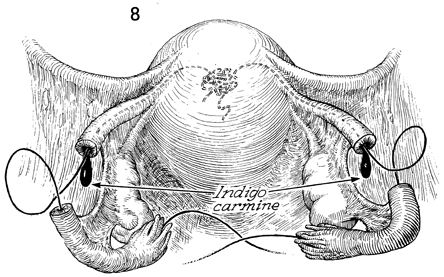
- Microresection and Microresection and anastomosis of the Fallopian tube are indicated in those cases of infertility where tubal obstruction has been diagnosed by hysterosalpingography and confirmed by laparoscopy. In recent years, this procedure has been performed by a microtechnique, utilizing fine suture and magnification with ocular loupes or an operating microscope. If careful hemostasis and microtechnique can be used, excessive postoperative scarring and peritubular adhesions can be reduced. Scarring and stricture formation at the site of the anastomosis can be minimized. This allows greater motility of the Fallopian tube, giving it a greater chance of receiving the oocyte, which is transported down the Fallopian tube to meet spermatozoa emerging from the proximal end of the tube. Physiologic Change. The Fallopian tube is restored to its normal function. Points of Caution. Meticulous hemostatic technique is essential. To ensure that a proximal portion of tube is patent, indigo carmine dye is injected via fine-gauge spinal needle placed through the fundus into the endometrial cavity, with the lower uterine segment obstructed with a clamp. The stent used to aid in performing the anastomosis is removed immediately after the operation. Technique
|
|||||||||||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.