|
||||||
|
Diagnostic Uses of Laparoscopy Demonstration of Tubal Patency via Laparoscopy Laparoscopic Resection of Unruptured Ectopic Pregnancy Ovarian Biopsy via Laparoscopy Electrocoagulation of Endometriosis via Laparoscopy Lysis or Adhesions via Laparoscopy Control of Hemorrhage During Laparoscopy Sterilization by Electrocoagulation and Division via Laparoscopy Silastic Band Sterilization via Laparoscopy Hulka Clip Sterilization via Laparoscopy Sterilization by the Pomeroy Operation Sterilization by the Modified Irving Technique Sterilization by the Minilaparotomy Technique Sterilization - Ucheda Technique Tuboplasty - Microresection and Anastomosis of the Fallopian Tube |
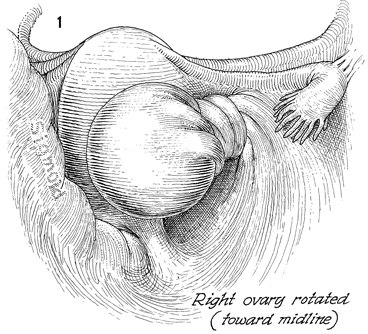
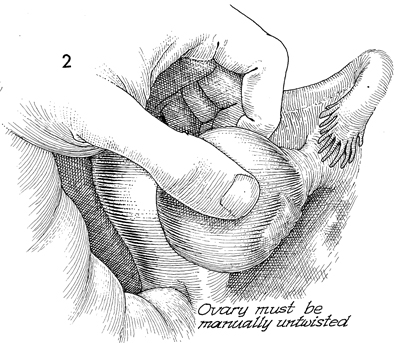
Torsion of Ovary Torsion of the ovary occurs when there is some additional weight acquired by the normal ovary, usually in the form of an ovarian cyst (physiologic or pathologic). Embryologically, the ovary is a retroperitoneal structure and invaginates an envelope of peritoneum that covers it and the stalk of the ovary commonly referred to as the infundibulopelvic ligament. This arrangement allows the ovary to undergo torsion. In most cases, the torsion turns toward the midline, i.e., the right ovary twists clockwise, and the left ovary twists counterclockwise. In the past, all such twisted ovaries were generally removed. It was accepted practice that the infundibulopelvic ligament be clamped prior to untwisting the ovary. Clamping the infundibulopelvic ligament first was said to prevent pulmonary embolism from the veins in the infundibuloplevic ligament. Very little data exists to confirm this point of view. In younger women of the reproductive age group and those women who have completed their families but would still enjoy the benefits of a functioning ovary, salvage of this twisted ovary becomes an important issue. An ovary that has undergone torsion can be untwisted safely without pulmonary embolism. This can be done through an open laparotomy or through laparoscopy. The ovary can be safely untwisted and observed for the integrity of the vascular supply. Physiologic Changes. The
obvious physiologic change and the greatest threat to the ovary through
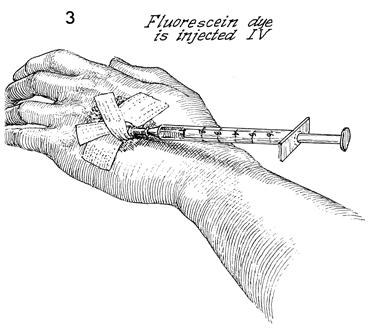
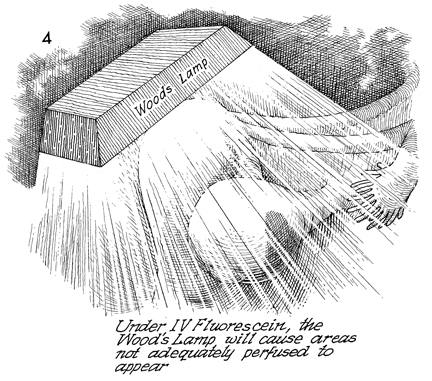
torsion is loss of blood supply. If the ovary can be salvaged, it can become a functional organ for the production of important estrogen and progesterone production as well as ovulation for those women who desire pregnancy. Points of Caution. The vascular integrity of the ovary must be demonstrated prior to completing the operation. Those ovaries that have undergone gangrene should be removed. The offending ovary cyst that produced the torsion in the first place should be excised. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.