|
|||||||
Diagnostic Uses of Laparoscopy Demonstration of Tubal Patency via Laparoscopy Laparoscopic Resection of Unruptured Ectopic Pregnancy Ovarian Biopsy via Laparoscopy Electrocoagulation of Endometriosis via Laparoscopy Lysis or Adhesions via Laparoscopy Control of Hemorrhage During Laparoscopy Sterilization by Electrocoagulation and Division via Laparoscopy Silastic Band Sterilization via Laparoscopy Hulka Clip Sterilization via Laparoscopy Sterilization by the Pomeroy Operation Sterilization by the Modified Irving Technique Sterilization by the Minilaparotomy Technique Sterilization - Ucheda Technique Tuboplasty - Microresection and Anastomosis of the Fallopian Tube |
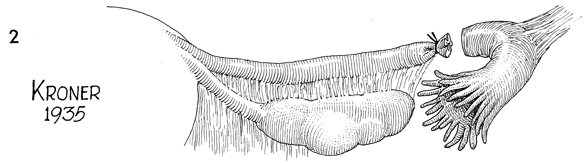
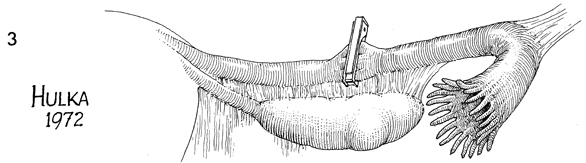
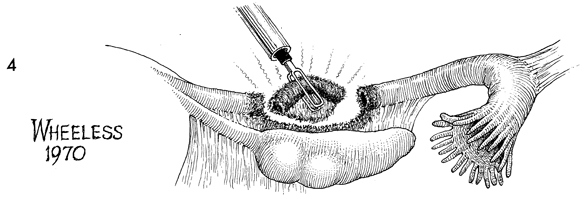
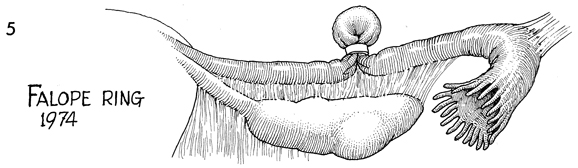
Fallopian Tube Sterilization Numerous Fallopian tube sterilization techniques are available to provide obstruction to the Fallopian tubes to prevent sperm and oocyte from fertilizing and being carried into the uterus. Obviously, with so many techniques available no one technique has satisfied all the criteria to come as close as possible to 100% effectiveness and be associated with a simple outpatient technique. No technique has been 100% successful. In general, most techniques have had a failure rate of 4 pregnancies/1000 patients operated on. Generally, failures have occurred with two techniques: recanalization of the Fallopian tube and development of a tuboperitoneal fistula. Most failures occur within the first 2 years of surgery, although they have been reported as late as 10 years following surgery. Successful tubal reanastomosis to allow pregnancy has been directly proportional to the amount of tube destroyed. Those sterilization operations that destroy the most Fallopian tube have the least successful pregnancy rate after reanastomosis, and those techniques that have the least tubal destruction have the best pregnancy rates after reanastomosis. Physiologic Change. There is little physiologic change to the patient following tubal obstruction. There has been no evidence that there is a change in sex steroid production by the ovary. Points of Caution. All sterilization procedures have reported morbidity to the gastrointestinal tract and the urinary tract from entering the abdominal cavity. Very little difference can be demonstrated by one technique versus another technique. Hemorrhage from the Fallopian tube secondary to the sterilization procedure does occur. Technique
|
||||||


Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.