|
||||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection of Unruptured Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
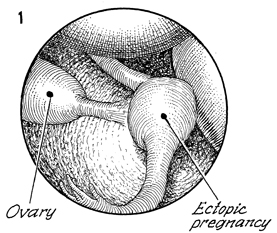
Laparoscopic
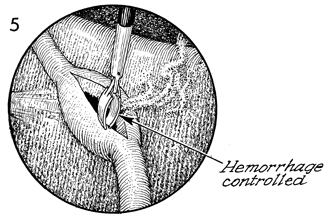
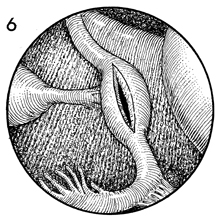
Resection of The laparoscopic resection of unruptured ectopic pregnancy has become
a useful and efficacious management of this problem that formally required
a pelvic laparotomy with a lengthy hospital stay. These patients usually
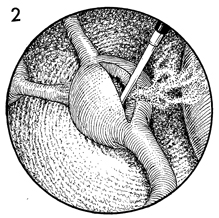
presented with the triad of amenorrhea, pelvic pain and vaginal bleeding. The laparoscope can be an additional diagnostic aid as well as a surgical treatment. Physiologic Changes. The
oocyte site has been impregnated with sperm, usually in the midportion
of the Fallopian tube. There are some physiologic factors present
that do not allow the new embryo to be taken down the tube and into
the endometrial cavity. These frequently range from a history of
inflammatory disease to external adhesions that obstruct the Fallopian
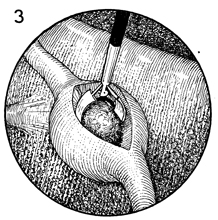
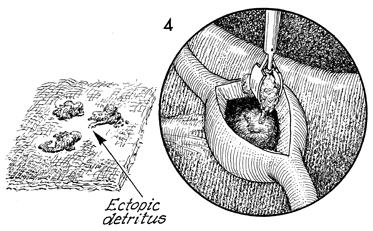
tube. Removal of the trophoblastic tissue from the tube immediately lowers the human chorionic gonadotropin levels in the blood. Points of Caution. Laparoscopy may be difficult in patients with a large ruptured ectopic pregnancy with copious bleeding. In these patients, laparoscopy is a waste of time. These patients should be treated with laparotomy. In certain cases, the surgeon may find that the serum chorionic gonadotropin levels have not fallen after laparoscopy. This may mean that all trophoblastic tissue has not been resected. If the patient is stable, treatment with methotrexate may be indicated. Technique
|
|||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.