|
||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
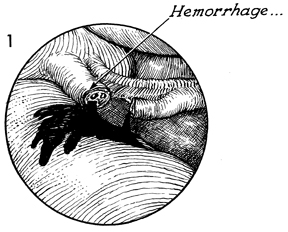
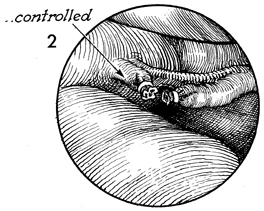
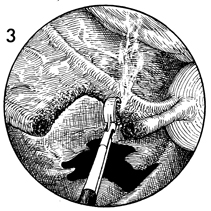
Control of Hemorrhage Hemorrhage secondary to laparoscopic procedures, particularly tubal
sterilization, can frequently be controlled via the laparoscope with
electrocoagulation and/or Silastic banding of the bleeding points. The purpose of this operation is to control bleeding. Physiologic Changes. Pelvic hemorrhage is controlled. Points of Caution. If bleeding occurs adjacent to a vital structure, the Silastic band technique is preferred over the electrocoagulation technique. The electrocoagulation technique is adequate, however, for control of hemorrhage on the Fallopian tube. Care must be taken to ensure that hemorrhage is controlled prior to withdrawing the instruments from the abdomen. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.