|
||||||
Appendectomy Using End Sigmoid Colostomy With Hartmann's Pouch Anterior
Resection Low
Anastomosis Anterior
Resection |
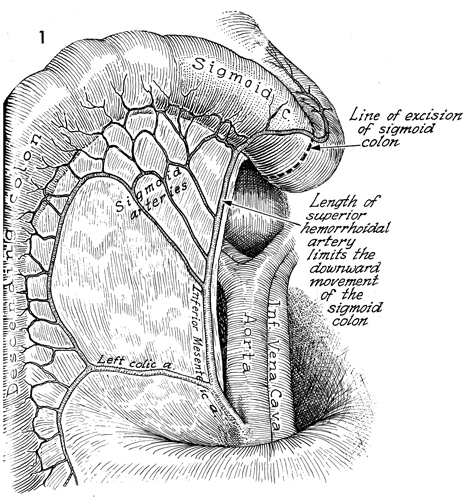
Anterior Resection of the Colon The Strasbourg-Baker technique allows side-to-end anastomosis of the sigmoid colon to the rectal stump without sacrificing the inferior mesenteric artery. It also usually allows preservation of the superior hemorrhoidal artery. It can be performed with the suture technique or the new EEA (end-to-end anastomosis) stapler. When the blood supply to the proximal colon has been compromised from pelvic irradiation or inflammatory disease of the bowel, the anastomosis between the colon and rectum may be compromised by inadequate blood supply. In this procedure, it is important that the sigmoid colon be of sufficient length to perform the anastomosis without sacrificing the superior hemorrhoidal branch of the inferior mesenteric artery. If both these arteries are sacrificed, the blood supply for the descending and sigmoid colon becomes dependent on the middle colic artery and the integrity of the marginal artery of the colon; and if the marginal artery has been compromised through inflammation or radiation, a portion of the sigmoid colon may become ischemic. Points of Caution. Adequate mobilization of the descending
colon must be achieved to prevent tension on the anastomosis. Occasionally,
the terminal branch of the superior hemorrhoidal artery may have to
be sacrificed to accomplish this. Care should be taken to retain as
many of the sigmoid artery branches of the inferior mesenteric artery
as possible to improve the blood supply to the terminal colon and the
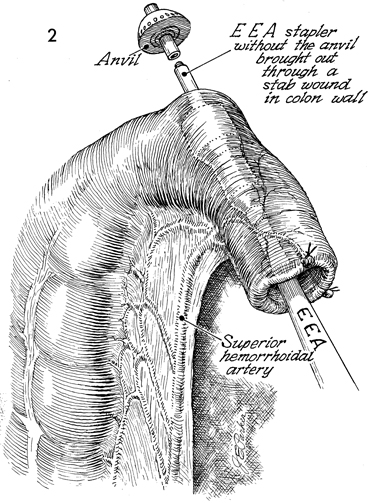
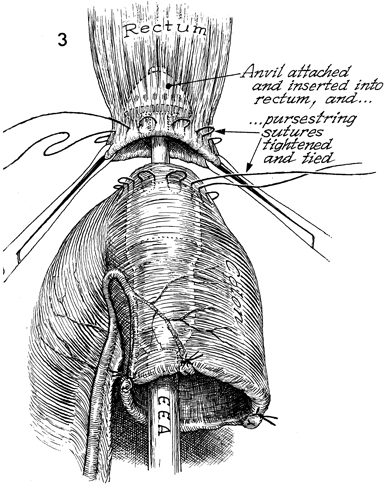
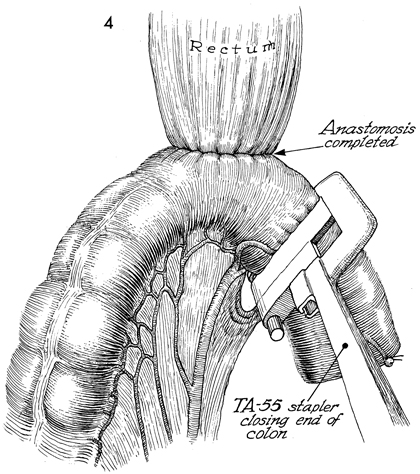
anastomosis. After achieving anastomosis with the EEA stapler, the surgeon should perform the three standard tests that confirm that an anastomosis is without defects: (1) the sterile sigmoidoscope should be inserted through the anus, and the anastomosis should be thoroughly inspected by visualization; (2) a small mount of air should be pumped into the rectum, and the pelvis should be filled with sterile saline solution-a stream of bubbles from the anastomosis indicates a defect; and (3) the two intact concentric rings of the bowel retrieved from the anvil of the EEA stapler should be observed. In resecting the excessive sigmoid colon distal to anastomosis by the EEA stapler, the surgeon must be careful not to inadvertently place the TA-55 stapler across the superior hemorrhoidal artery or one of its main branches. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.