|
||||||
Abdominal
Wound Massive
Closure Hemorrhage Control Following Laceration |
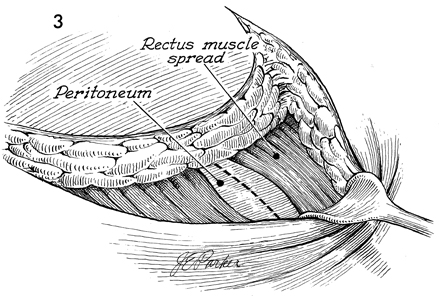
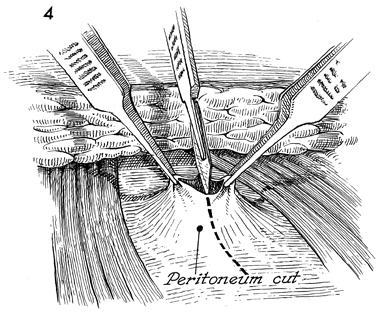
Pfannenstiel Incision The Pfannenstiel incision has become popular in the past decade for cosmetic reasons. This is particularly true in younger women having surgery for benign gynecologic and pelvic problems. If properly placed, it is generally concealed by regrowth of pubic hair. The purpose of the technique is to provide a cosmetic incision for pelvic surgery. Physiologic Changes. The Pfannenstiel incision transects neurovascular pathways in the skin of the abdominal wall and frequently requires partial or compete transection of the rectus abominis muscle. It is rarely associated with incisional hernia, has a low incidence of wound dehiscence, and heals without significant scarring. The latter fact may be due to the copious blood supply in the mons pubis. Points of Caution. A Pfannenstiel incision should never be used in oncologic surgery. It does not give exposure to the upper abdomen and provides only limited exposure to aortic and lymph nodes for their analysis and dissection. Care must be taken to avoid incidental laceration of the inferior epigastric artery and vein on the lateral margin of the rectus muscles. If the muscles are to be transected, the epigastric artery and vein should be identified, clamped, and ligated prior to transection of the muscle. In addition, care should be taken with regard to the point of entry into the peritoneum. If the incision is made too low, the bladder can be entered. Hemostasis is particularly important during this incision. The vascularity of the mons pubis increases the risk of hemorrhage, formation of hematoma, and infection. The surgeon should ensure that the incision is dry before closure of the wound. If there is any question, a small suction drain should be left in the incision for 24-48 hours. Technique
|
|||||


Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.