|
||||||
Abdominal
Wound Massive
Closure Hemorrhage
Control Following Laceration |
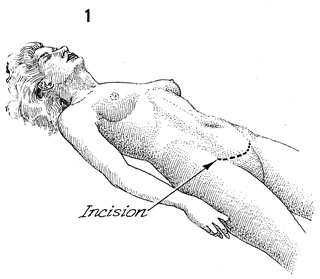
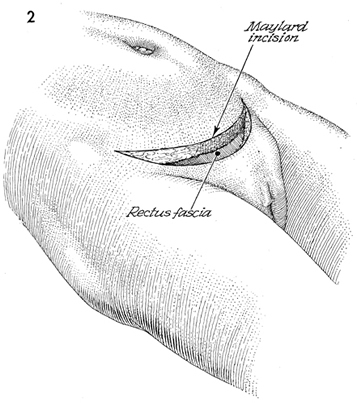
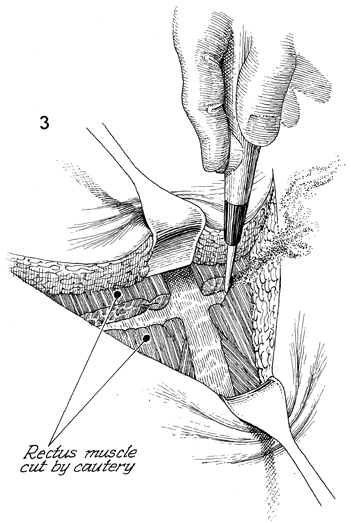
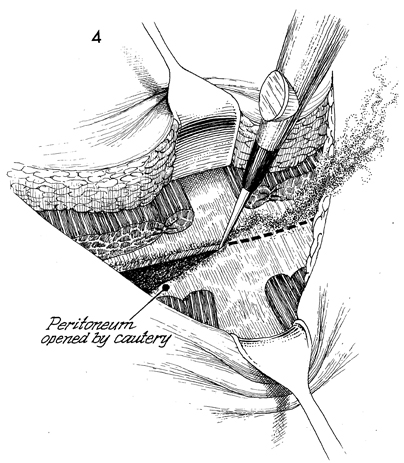
Maylard Incision The Maylard incision is an abdominal incision that can afford extensive exposure to the pelvic organs when this is needed. Although it can be used for most gynecologic procedures, it is not particularly useful in such upper abdominal surgeries as ovarian cancer that may be associated with tumor in and around the liver or spleen. Its main disadvantage is that it is a more painful incision for the patient during the first postoperative week. This may be weighed against its reduced rate of incisional hernia and the fact that it is cosmetically advantageous, since it does not scar the midabdomen. Physiologic Changes. None. Points of Caution. Care must be taken to ensure the integrity of the ligature on the inferior epigastric artery lateral to the rectus fascia. We prefer a sloping U-shaped incision from the anterior superior iliac spine down slightly superior to the mons pubis to the superior iliac spine on the opposite side. This course should definitely be marked on the patient with brilliant green solution prior to making the incision. Technique
|
|||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.