|
||||||||
Abdominal
Wound Massive
Closure Hemorrhage
Control Following Laceration |
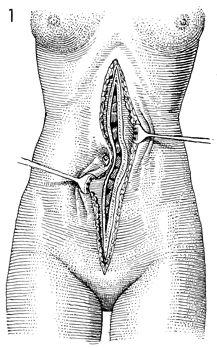
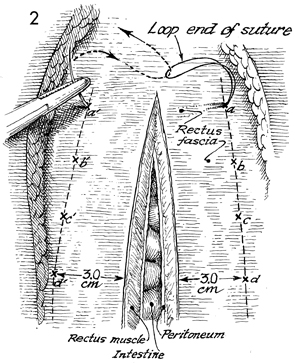
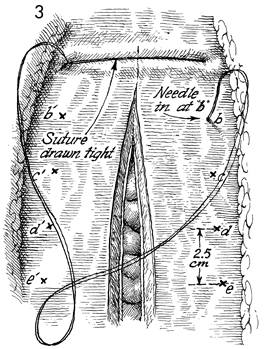
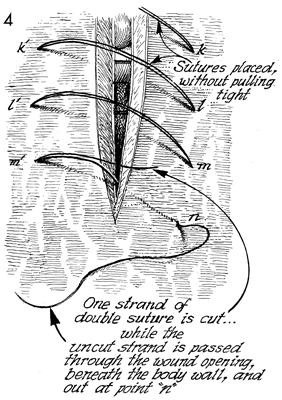
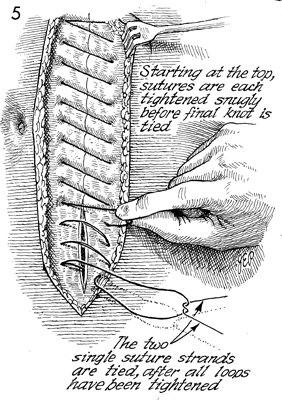
Massive Closure Techniques for closure of the midline abdominal incision have varied over time with better understanding of the physiology and engineering of closure of the abdominal wall and changes in materials in surgical suture. Closure of the midline through multiple layers including (1) the peritoneum and (2) the edges of the rectus fascia has evolved from braided products such as silk and cotton to synthetic braided products such as Teflon and braided nylon. Contemporary surgical data show that closure of the peritoneum in a single layer in the pelvis or on the abdominal wall is unnecessary. Engineering sciences applied to wound healing have shown that the interrupted sutures have a weaker suture line than do running sutures. The weakest point in any suture line is the knot. Therefore more knots equal a weaker suture line, and less knots equal a stronger suture line. With the advent of delayed synthetic absorbable sutures, especially monofilament sutures, an entire abdominal midline incision from xiphoid to symphysis can be closed with the mass closure technique utilizing one knot. Physiologic Changes. The physiology and engineering of this suture rely on the give and take of a suture line or cable line in any situation where total fixation of a suture through tissue with movement results in a "giggly saw" technique of tearing the tissue. Mass closure with the one-knot loop suture technique allows give of the suture with coughing, respiration, and movement. It basically holds the wound together and allows the properties of wound healing, the strongest of all wound-healing techniques, to take place without necrosis and closure by second intention. Points of Caution. Monofilament suture should be used. Most wounds can be completely closed with delayed monofilament synthetic suture. There may be a place for monofilament synthetic permanent suture such as nylon or Prolene. The loop suture eliminates all the knots except one. Care must be taken to allow a 3-cm margin, wider than a man's finger, and to place the sutures 2 1/2 -3 cm apart. These characteristics of the length and width of the mass closure are necessary to conform to engineering principles. Technique
|
|||||||


Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.