|
||||||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
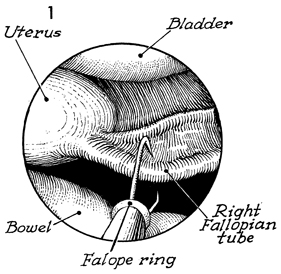
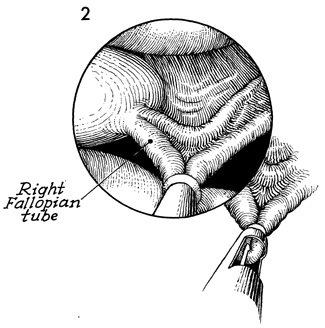
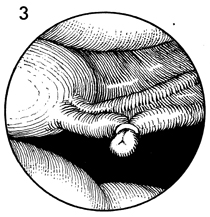
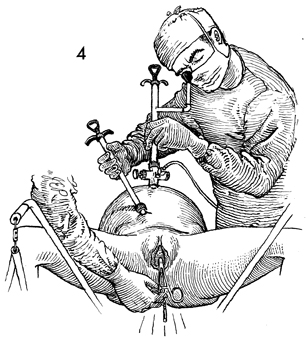
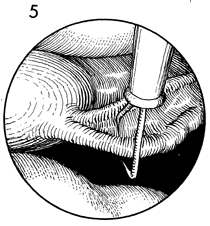
Silastic Band Sterilization The Fallopian tube can be adequately obstructed by the application of a Silastic band to a knuckle of Fallopian tube. This produces necrosis of the tube from ischemia and, thereby, causes tubal obstruction. It has an advantage over the electrocoagulation technique in that it is equally successful, statistically, preventing pregnancy and avoids the possibility of electrothermal burns. The purpose of the Silastic band applied by laparoscopy is to obstruct the Fallopian tube to achieve female sterilization. Physiologic Changes. The Fallopian tubes are obstructed. Points of Caution. Care must be taken not to bring an excessively large knuckle of Fallopian tube into the housing of the banding scope. If a large mass of Fallopian tube, with associated mesosalpinx, is brought into the housing of the laparoscope, the grasping tongs will lacerate the tube. Technique
|
|||||||||


Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.