|
||||||||||
|
Diagnostic Uses of Laparoscopy Demonstration of Tubal Patency via Laparoscopy Laparoscopic Resection of Unruptured Ectopic Pregnancy Ovarian Biopsy via Laparoscopy Electrocoagulation of Endometriosis via Laparoscopy Lysis or Adhesions via Laparoscopy Control of Hemorrhage During Laparoscopy Sterilization by Electrocoagulation and Division via Laparoscopy Silastic Band Sterilization via Laparoscopy Hulka Clip Sterilization via Laparoscopy Sterilization by the Pomeroy Operation Sterilization by the Modified Irving Technique Sterilization by the Minilaparotomy Technique Sterilization - Ucheda Technique Tuboplasty - Microresection and Anastomosis of the Fallopian Tube |
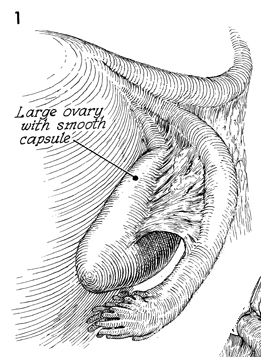
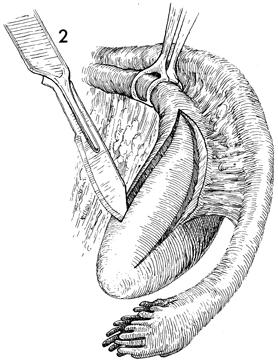
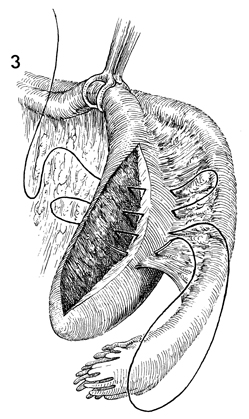
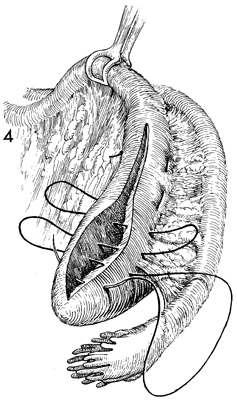
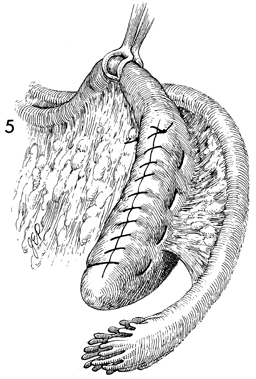
Wedge Resection of the Ovary Wedge resection of the ovary is most often performed in the treatment of polycystic ovary syndrome (Stein-Leventhal). After appropriate gynecologic and endocrinologic evaluation and after all possible medical therapy with estrogen antagonists has failed, wedge resection may be the procedure of choice to induce ovulation and menstrual periods. Physiologic Changes. The precise mechanism for the induction of ovulation by wedge resection of the ovary is not known at this time. There are two possible explanations for this physiologic change: (1) the hyperplastic ovarian capsule is removed, thereby mechanically allowing ovulation, and (2) the mass of ovary is reduced, thus shifting the ratio between the level of pituitary gonadotropin and the mass of the ovary in such a way as to favor induction of ovulation. Points of Caution. There are two important points of caution of this operation: (1) the control of hemorrhage from the biopsy site in the ovary and (2) the reduction in the peritublar adhesion formation associated with wedge resection of the ovary. Therefore, fine meticulous technique must be utilized if peritubular adhesion formation is to be avoided. Technique
|
|||||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.