|
||||||||
Diagnostic
Uses Demonstration Laparoscopic
Resection Ovarian
Biopsy Electrocoagulation
of Lysis
or Adhesions Control
of Hemorrhage Sterilization
by Silastic
Band Sterilization Hulka
Clip Sterilization Sterilization
by the Sterilization
by the Sterilization
by the Sterilization - Ucheda Technique Tuboplasty
- |
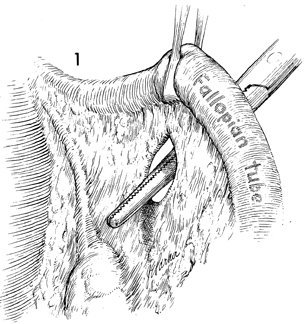
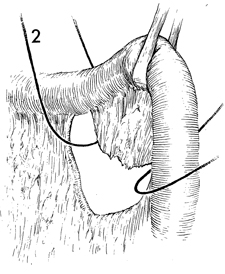
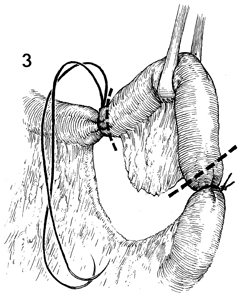
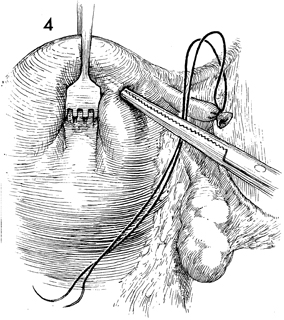
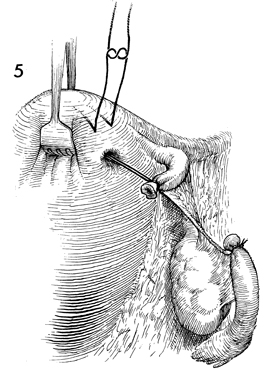
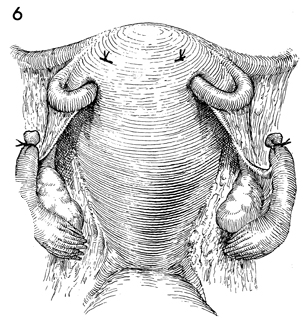
Sterilization by the Modified The modified Irving operation was proposed to prevent the small but persistent incidence of failures associated with the Pomeroy procedure. Although prospective randomized studies are unavailable at this writing, this operation is regarded as one of the most effective for prevention of pregnancy. The purpose of the procedure is to prevent pregnancy by obstructing the Fallopian tubes by burying their proximal portions back into the myometrium. Physiologic Changes. The physiologic changes with the modified Irving technique are similar to those associated with the other methods of tubal obstruction and ligation. In addition, the proximal portion of the Fallopian tube is buried within the myometrium. This makes recanalization or the development of a tuboperitoneal fistula extremely unlikely. Points of Caution. An adequate opening in the myometrium must be made with the straight mosquito clamp if the Fallopian tube is to be pulled within the myometrium. Technique
|
|||||||

Copyright - all rights reserved / Clifford R. Wheeless,
Jr., M.D. and Marcella L. Roenneburg, M.D.
All contents of this web site are copywrite protected.